Obesity has become a global epidemic and represents a major public health challenge (1). According to the World Health Organization (WHO), approximately 1 billion people worldwide are living with obesity (BMI ≥30), while 2.5 billion adults aged 18 years or older are classified as overweight (2). Obesity is a complex, chronic, and relapsing disease characterized by excessive adipose (fat) tissue accumulation (2,3), resulting from both fat cell (adipocyte) enlargement (hypertrophy) and increased adipocyte number (hyperplasia) (4). There are serious comorbidities associated with obesity, including type 2 diabetes (T2D), cardiovascular disease, musculoskeletal disorders, and sleep apnea, to name a few (5–7). One of the root causes of obesity is the long-term imbalance between energy intake and expenditure. However, there are many factors that contribute to obesity, including insulin resistance, cortisol imbalance, consumption of processed food, processed sugars (saccharose, fructose syrup), and alcohol intake accompanied by a sedentary lifestyle (Figure 1). Signals of hunger and satiety are communicated to the brain through neuronal and humoral pathways originating from peripheral organs, including the gastrointestinal tract, pancreas, and adipose tissue, which regulate food intake, nutrient processing, and energy storage (8).

Glucagon-like peptide-1 (GLP-1) has been recognized as one of the key regulators of gut-to-brain signaling involved in the control of food intake and satiety. Mechanistically, GLP-1 lowers blood glucose by stimulating glucose-dependent insulin secretion, while also slowing gastric emptying and promoting satiety, thereby reducing food intake and contributing to weight loss (8, 10). GLP-1 receptor agonists (GLP-1RAs) have been developed to treat obesity and type 2 diabetes by pharmacologically activating GLP-1 signaling, thereby modulating central nervous system (CNS) pathways that reduce food intake and promote weight loss (9). Several FDA-approved medications are currently available for the treatment of obesity, including widely used injectable therapies such as Zepbound (tirzepatide) and Wegovy (semaglutide), as well as recently approved oral medication Foundayo (orforglipron). Many additional molecules are currently undergoing clinical trials, with increasing emphasis on the development of orally administered therapies. Clinical studies in individuals with obesity have demonstrated substantial efficacy, with semaglutide, tirzepatide (11), and orforglipron (12) producing mean body-weight reductions of approximately 12%, 18%, and 11.2%, respectively. Growing interest in weight-loss medications was reflected in an almost 600% increase in GLP-1 receptor agonist prescriptions between 2020 and 2023, raising important questions and concerns about the potential effects of their widespread use on human physiology and disease (13).
There are several concerns regarding the use of GLP-1 therapies, which are not currently widely discussed. Real-world evidence (RWE) suggests that the efficacy of these treatments is substantially lower than that observed in clinical trials because (a) patients often do not strictly adhere to prescribed treatment regimens and (b) medication-related side effects may lead to dose reductions or treatment discontinuation. Some of the common side effects include gastrointestinal issues, including nausea, vomiting, pancreatitis, and diarrhea (14). An incredible 70% of patients treated with Semaglutide and Tirzepatide reported serious adverse events associated with gastrointestinal (GI) disorders (15). In addition, the long-term effects of GLP-1 receptor agonist use remain insufficiently studied (14), and their potential impact on human health over time is not yet fully understood. Moreover, current evidence suggests that many patients rapidly regain a substantial proportion of the weight lost after discontinuing GLP-1 receptor agonist treatment, with much of the regained weight consisting of fat mass (16–18).
So, the questions are: 1) Is it worth getting medicated? 2) Can we reduce/regulate our bodies without medication? 3) Are we just lazy?
Losing weight can provide significant health benefits for individuals who are overweight or have obesity. The goal should be to achieve and maintain a healthy body weight, generally corresponding to a BMI between 18.5 and 24.9 according to the WHO (2). But too many people nowadays prefer to get medicated to quickly lose weight, even before trying to modify their lifestyle, citing reasons such as: a) my body cannot lose weight — I tried; b) I don't have time for this; c) I cannot make significant changes to my work or lifestyle; or d) It's costly, and I don't have the finances to cope with that. Personally, I also found it difficult or impossible at the beginning to lower my body weight, blaming all these reasons. But the real reasons were completely different.
One of the main reasons people struggle to lose weight is a limited understanding of the underlying biology and how the body regulates energy balance, despite the abundance of information now available through healthcare and nutrition professionals, online resources, and printed materials. The biology is actually not that complicated, and the equation of lower calorie intake = body weight reduction over time works. However, the process is much more efficient if you allow two key hormones (insulin and cortisol), which are involved in human metabolism, to do their jobs. So, the goal is to increase or regain insulin sensitivity and balance cortisol levels. Plenty of literature is available on what food promotes (low glycemic fruits, vegetables, lean meat, and dairy) or negates (processed food, fatty meats, alcohol, and processed sugar) insulin sensitivity. The effect of cortisol on weight management is less discussed than that of insulin, but it also plays an important role when you are trying to lose or control your body weight. Therefore, regular sufficient sleep accompanied by light physical exercise and free-time activities contributes to well-balanced cortisol levels.
But I hear very often that:
- I don't have an extra 2–3 hours a day to go to the gym
- I hate doing cardio
- I don't like lifting weights
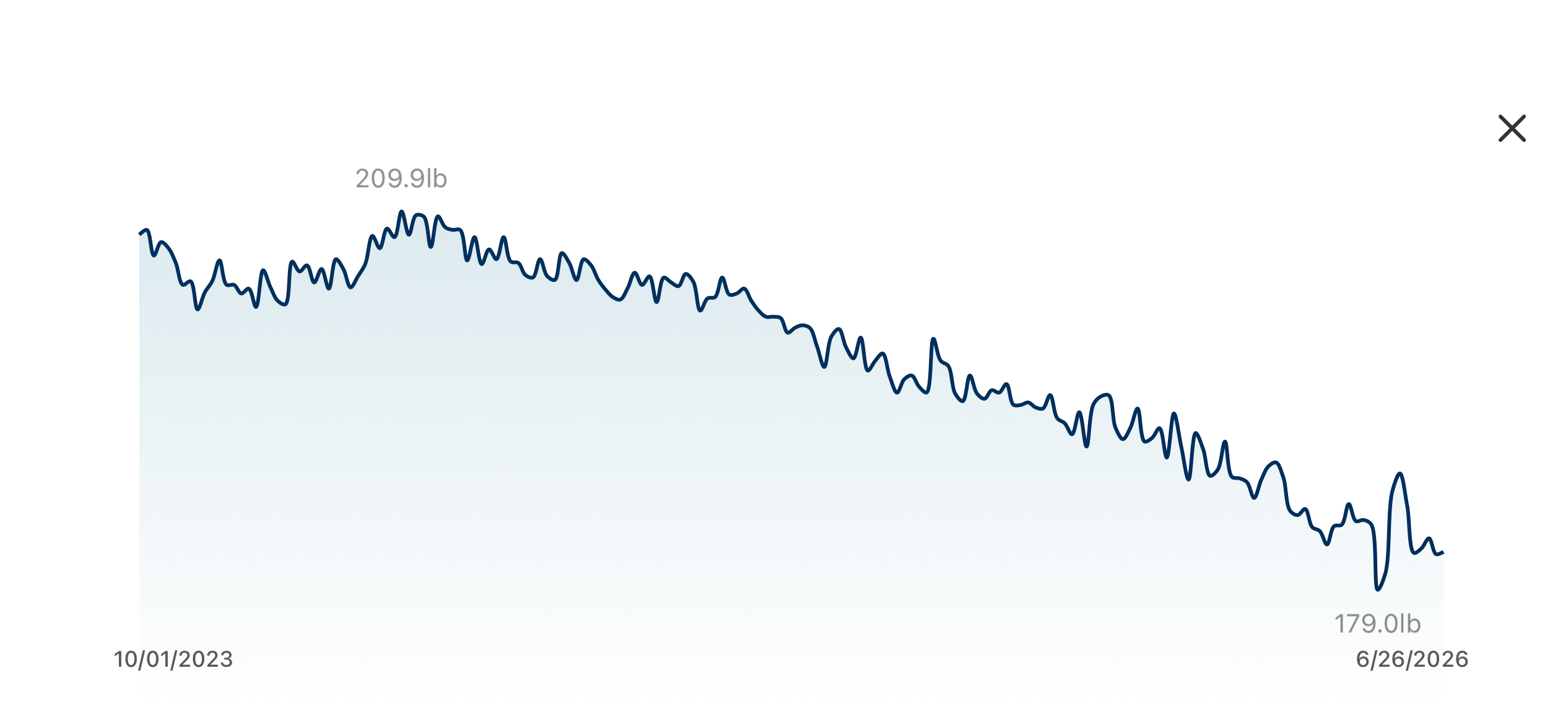
What if I told you that just 15–20 minutes of light exercise a day — without cardio or heavy weightlifting — could help reduce your body weight by 15%, potentially making it even more effective than Wegovy (semaglutide)? Would you consider it? Don't you believe it? Below is my body weight record over time, showing 30 pounds (15%) of body weight loss achieved without any medication, and avoiding (a) side effects associated with weight-loss medication and (b) the cost of those drugs, which are not cheap. I achieved this by modifying my diet to maximize insulin sensitivity and balance cortisol levels.
Another common misconception regarding physical activity is the belief that you must do a lot of cardio to lose or control your body weight. The truth is that cardio and high-intensity training are exercises that most efficiently burn calories. However, those exercises usually make you (a) tired quickly, (b) affect your joints, and (c) quickly burn calories, resulting in the body sending hunger signals to the brain, which, if you don't control, might negate the effort. Don't think that's true? Have you ever wondered why you don't see bodybuilders doing extensive cardio, but they all look lean? Because the "lean" factor does not come from doing cardio — it comes from the diet!
The last important point is that, as shown in the graph above, my body weight has been pretty much stable with 2–3 pounds of fluctuation, which is normal, and I did not regain the weight that is very often observed after the discontinuation of GLP-1-based therapies. Let me know what you think, or feel free to ask me any questions you have.

References:
- Ahmed et al. Adipose tissue and insulin resistance in obese. Biomed Pharmacother. 2021
- World Health Organization. Obesity and overweight 2025
- Frühbeck G, et al. The ABCD of obesity: An EASO position statement on a diagnostic term with clinical and scientific implications. Obes Facts. 2019
- Bluher M. Adipose tissue dysfunction in obesity. Exp. Clin. Endocrinol. Diabetes 2009
- Guh et al. The incidence of co-morbidities related to obesity and overweight: A systematic review and meta-analysis. BMC Public Health. 2009
- Gribsholt et al. Mortality among Danish patients with a hospital diagnosis of overweight or obesity over a 40-year period. Clin Epidemiol. 2022
- Valenzuela et al. Obesity and the risk of cardiometabolic diseases. Nat Rev Cardiol. 2023
- van Bloemendaal et al. Effects of glucagon-like peptide 1 on appetite and body weight: Focus on the CNS. J Endocrinol. 2014
- Blüher M. Obesity: global epidemiology and pathogenesis. Nature Reviews Endocrinology. 2019
- Holst J. The physiology of glucagon-like peptide 1. Physiological Reviews 2007
- Ghusn et al. Glucagon-like Receptor-1 agonists for obesity: Weight loss outcomes, tolerability, side effects, and risks. Obesity Pillars 2024
- Wharton et al. ATTAIN-1 Trial Investigators. Orforglipron, an Oral Small-Molecule GLP-1 Receptor Agonist for Obesity Treatment. N Engl J Med 2025
- Lee J. et al. Dispensing of Glucagon-Like Peptide-1 Receptor Agonist to Adolescents and Young Adults, 2020-2023. JAMA. 2024
- Thomsen et al. Real-world evidence on the utilization, clinical and comparative effectiveness, and adverse effects of newer GLP-1RA-based weight-loss therapies. Diabetes Obes Metab. 2025
- Fahim et al. Comparative safety and side effects of semaglutide and tirzepatide: Implications for clinical decision-making in obesity management. Biomed Pharmacother. 2025
- Wilding et al. Weight regain and cardiometabolic effects after withdrawal of semaglutide: the STEP1 trial extension. Diabetes Obes Metab. 2022
- Rubino et al. Effect of continued weekly subcutaneous semaglutide vs placebo on weight loss maintenance in adults with overweight or obesity: the STEP 4 randomized clinical trial. JAMA. 2021
- Aronne et al. Continued treatment with tirzepatide for maintenance of weight reduction in adults with obesity: the SURMOUNT-4 randomized clinical trial. JAMA. 2024